알츠하이머성 치매환자의 한글 철자 지식
Orthographic Knowledge of Hangul Syllable in Alzheimer’s Disease
Article information
Abstract
Objectives:
Alzheimer’s disease (AD) can cause visuoconstructional and linguistic dysfunction due to bilateral involvement of the tempoparietal-frontal hemispheric areas. At the later stages of disease, the patients often manifest written language impairment. Generalized orthographic knowledge/representation, that is, knowledge of symbol and letter patterns within and across words, is important for written language. The aim of this study was to delineate the basic knowledge of the graphemic or syllabic shapes in Hangul as well as Hangul writing ability of those with AD. We hypothesized that the orthographic representation of Hangul syllable might withstand the impact of AD, because the basic knowledge of a letter shape of Hangul might be preserved in this clinical population.
Methods:
Seventy-five AD patients were included in this study. The patient group was divided into four subgroups according to the clinical dementia rating (CDR): 16 were very mild cases (CDR0.5); 37, mild (CDR1); 19, moderate (CDR2); and 3, severe (CDR3). We administered dictation and representation tasks of Hangul syllables and compared the performances among groups.
Results:
In the writing-to-dictation and representation tasks, the number of correct responses significantly differed according to CDR (p<.001). Interestingly, the patients at a later stage of the disease received scores of below 10% on the Hangul writing to dictation task, and 41.5% on the Hangul representation tasks.
Conclusion:
This finding supports the hypothesis that orthographic knowledge/representation of Hangul grapheme/syllable may partly withstand the impact of AD.
Normal spelling and writing can be performed with an ensemble of intact skills including visuospatial orientation, construction, and linguistic capacities. Generalized orthographic knowledge/ representation, that is, knowledge of symbol and letter patterns within and across words, is also important for written language (Kaefer, 2009).
Alzheimer’s disease (AD) is a disease that can result in both visuoconstructional and linguistic dysfunction during the course of the disease, due to bilateral involvement of the tempoparietal-frontalhemispheric areas. AD patients usually manifest writing impairment. Previous studies on Korean AD patients showed that writing impairments are closely related to functional decline in both the right and left hemispheres (Yoon et al., 2011, 2012).
The Korean alphabet, Hangul (or Hangeul), is composed of uniquely shaped letters. In terms of syllabic forms, the English alphabet is always arranged in a linear string fashion from left to right. What makes the Hangul syllable so unique is that it can be arranged vertically, horizontally, and with a combination of thetwo. Each consonant(s) and vowel(s) needs to be arranged in a square form, which represents one syllable. In addition, in the physical forms of graphemes, the ten basic vowels are derived from three basic geometric shapes, which represent the three fundamental elements in Eastern cosmology (i.e., heaven, earth, and humanity). The consonants are modeled after pictorial vocal representations. For example, ‘ㄱ/g/’ depicts the root of the tongue blocking the throat.
Research on the knowledge of the graphemic or syllabic shapes in Hangul as well as the characteristics of Hangul writing would provide additional information for non-alphabetic written language systems. To date, the hypothesis that Hangul writing contains not only linguistic but also visuospatial characteristics, has been confirmed in Korean stroke (Kim, Na, & Park, 2007) and AD patients (Yoon et al., 2011, 2012). However, studies on the characteristics of orthographic representation in Hangul are very limited. With respect to the visuospatial representation of syllabic shape of Hangul writing, Kim, Na, & Park (2007) proposed that the representation of Hangul syllabic shape remained intact despite the cerebrovascular disease. In a similar token, studies on English and Italian-speaking adults showed rigid positions of vowel-consonant status in a word (Glasspool & Houghton, 2005; Miceli, Capasso, Benvegnu, & Caramazza, 2004).
Orthographic representation is a basic element of reading and writing processes. Lavine (1977) and Bialystok (1995) suggested that young pre-school children possess some orthographic knowledge. When 5year old children were presented with different types of printed stimuli, they were able to label printed words and pseudowords as writing. The aim of this study was to delineate the basic knowledge of the graphemic or syllabic shapes in Hangul as well as Hangul writing ability of those with AD. We hypothesized that the orthographic representation of Hangul syllable might withstand the impact of the AD because the basic knowledge of a letter shape of Hangul might be preserved in the clinical population.
METHODS
Subjects
Seventy-five AD patients in a previous study (Yoon et al., 2012) were also included in this study. All patients fulfilled the criteria, proposed by the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA), for having probable AD (McKhann et al., 1984). The exclusion criteria were as follows: 1) with less than “6 years of education”, for they might have had difficulty writing Hangul in the premorbid state; 2) who showed abnormal findings on laboratory tests (i.e., a complete blood count, blood chemistry, vitamin B12/folate, syphilis serology, thyroid function tests); 3) showing territorial cerebral infarctions, brain tumors, and other structural lesions on magnetic resonance image; 4) with mild bradykinesia and rigidity that can influence writing ability; and 5) who refused to complete the Hangul writing and representation tests. The patient group was divided into four subgroups according to the clinical dementia rating (CDR): 16 were very mild cases (CDR0.5); 37, mild (CDR1) 19, moderate (CDR2); and 3, severe (CDR3). Table 1 presents demogrpahic variables according to the disease severity.

Demographic variables according to the disease severity
Materials
Hangul writing to dictation task
Performance on a Hangul writing to dictation task was conducted to identify the writing ability of the patients. The writingtask consisted of 60 single syllable characters. The selection of these particular characters as stimuli was based on configuration, frequency, and imageability. In terms of configuration, characters with four graphemes or less were selected to make the task less complicated. In terms of vocabulary frequency, words were selected from the frequently used words in the Learner’s Dictionary of Korean (Seo, 2006). All words were concrete, to ensure high imageability. The stimuli are provided in the Appendices 1-3.
Hangul representation task
The aim of the orthographic representation task of Hangul was to assess the knowledge of the shape of a real Hangul grapheme and syllable. In this scenario, we created the pseudo-shaped graphemes and syllables as distracters which were not included in the Korean syllable inventory. This task was divided into two subcategories: the first subtask included 10 yes-no questions and the second included 10 four-choice test items. Real and pseudo-shaped graphemes and syllables belonged to the stimuli. The stimuli are provided in the Appendix.
Language test
All patients completed the Korean version of Western Aphasia Battery (WAB; Kim & Na, 2004). The oral language subtests such as spontaneous speech, auditory comprehension, repetition, and naming are used to calculate the aphasia quotient (AQ). When the reading and writing scores are added, the language quotient (LQ) is obtained. The patients with AD exhibited a mean AQ of 82.1 and a LQ of 76.5 (maximum score=100). Table 2 shows the resultsof the language test according to the dementia disease severity.

The results of the language test according to the dementia disease severity
Procedure
For the Hangul writing to dictation task, we requested the subjects to write on an A4-sized sheet of paper. Each Hangul stimulus was verbally presented to the patient with a word cue; for example, “Please write the syllable ‘가’ (/ka/) of ‘가위’ (/kawi/).” The subject was asked to verbally repeat the target stimulus before writing it to ensure that the stimuli were correctly understood.
The Hangul representation task did not require the written production of the syllable or the verbal description. As mentioned earlier, this task was divided into two subcategories. The first subtask was a form of yes-no questionnaire. Here, the subjects were shown one stimulus printed on a sheet. The instruction was “Try to judge if the shapes of the written Hangul syllables are correct or not.” The second subtask consisted of multiple choice test items. The general principle of this subtask involved pointing to the correctly shaped syllable among four multiple-choice items. The instruction was “Point the correctly shaped Hangul syllable.” The subjects first performed a practice item (‘가’).
Analysis
Hangul writing to dictation task
The number of the correctly produced Hangul syllables was counted. We assigned a score of “1” if the patient showed correct responses of all grapheme in a syllable, and a score of “0” for an incorrect or no response. The maximum score was 60 and the minimum, 0.
Hangul representation task
We assigned a score of “1” and “0” for correct and incorrect responses, respectively. The maximum score was 20.
Statistics
One-way analysis of variance and post hoc Bonferroni correction were conducted to identify differences according to disease severity within the AD group regarding the number of correct responses.
RESULTS
In the writing to dictation task, the number of correct responses significantly differed according to CDR (p<.001) (Table 3). By comparing the mean number of correct responses among the patient groups, there were significant differences between CDR0.5 and CDR2, CDR0.5 and CDR3, CDR1, and CDR2, and between CDR1 and CDR3. No differences were observed between CDR0.5 and CDR1, and between CDR2 and CDR3 (p<.05).
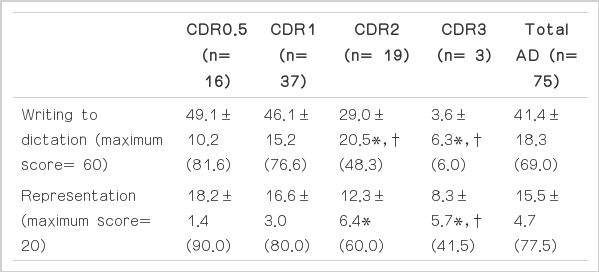
The mean number and percentage (%) of correct responses of writing to dictation task and Hangul representation task
In the representation task, the number of correct responses significantly differed according to CDR (p<.001) (Table 3). There were significant differences of the correct responses between CDR- 0.5 and CDR2, CDR0.5 and CDR3, and between CDR1 and CDR3 (p<.05).
In the early stage of disease (CDR0.5 and CDR1), the patients showed correct responses above 75% in both writing to dictation and Hangul representation tasks. The CDR2 group showed correct responses below 50% in Hangul writing to dictation task, but the Hangul representation was preserved with 60% of accuracy in the group. The CDR3 patients showed correct responses below 10% in Hangul writing to dictation task, and could manifest 41.5% of accuracy in Hangul representations.
CONCLUSION
We hypothesized that the orthogrpahic representation of Hangul syllable might withstand the impact of AD because the knowledge of a letter shape of Hangul might be preserved in the clinical popoulation. The primary finding from this study was that the later stages of AD affects the orthogrpahic representation of Hangul less than Hangul writing ability.
Typically, patients with severe stages of AD experienced more problems with linguistic and motoric components in writing, and showed more errors in writing to dictation (Forbes, Shanks, & Ven neri, 2004; Neils-Strunjas, Shuren, Roeltgen, & Brown, 1998; Platel et al., 1993). In our group of late stages of AD, the patients also showed more errors and the performance showed scores of below 10% in the Hangul writing to dictation task. Based on the subscore of the reading test of WAB, these CDR3 patients could not read aloud or understand context well (the reading score=3.0± 3.5). However, they manifested 41.5% of accuracy in the Hangul representation tasks. On the other hand, for those in the early stage of AD (CDR1), the performance showed scores above 75% in both writing to dictation and the Hangul representation tasks. In this stage, the abilities to write and recognize the Hangul syllable are similar. In short, a higher discrepancy between the performance of writing and representation tasks was observed in CDR3.
The explanation for these phenomena is two-fold. Firstly, the representation task requires relatively less higher cognitive processes. In this task, the subjects only had to discern and point to the correctly shaped syllable in the form of a yes-no questionnaire and four multiple-choice items, respectively. It did not require written production of the syllable or verbal description. However, writing to dictation is a high-level, complex, cognitive process and requires a series of steps (e.g., neuropsychologic and motor functions) for its successful execution. Jauk, Benedek, & Neubauer (2012)mentioned that divergent behavior involves the use of broad search of cognitive storage whereas convergent behavior involves a narrow search of the storage. In this point of view, the Hangul representation task as a convergent task is a straightforward method whereas the writing to dictation task may be a divergent task. Thus, our finding may be ascribed to the fact that the deficits in the divergent task worsen with progression of the disease.
Secondly, it can be assumed that the early acquired orthographic representation/knowledge of Hangul grapheme/syllable might be preserved in the later stage of AD. The orthographic representation/ knowledge is acquired in the very early stages of development (Frith, 1986; Kaefer, 2009). There was evidence that prereading children can show orthographic knowledge. Retrogenesis can be defined as the process by which degenerative mechanisms mirror the inverse sequences of the maturation process of normal development (Reisberg et al., 2002). Kim et al. (2011) observed that AD patients tend to first lose words learned more recently while maintaining those learned during earlier stages of development. From the aspect of retrogenesis (Kim et al, 2011; Reisberg et al., 2002), early acquired orthographic knowledge of Hangul grapheme/ syllable might be at least partially, if not totally, remained in the minds of Korean AD patients even though they lack abilities to read and write. However, impairment of the basic knowledge of language, as writing ability is finally disrupted, might be also detected in the terminal stage of AD.
This study is noteworthy because this is the first attempt to describe orthographic knowledge of Hangul in patients with AD. Limitations and suggestions of the study are as follows. With respect to sample size for the later stage of AD (i.e., CDR3), the number of subjects was not large enough to allow safe conclusions to be drawn, so future studies are needed to clarify the results. In the future, we would like to investigate whether the preservation of orthographic knowledge is restricted to Hangul, or whether it also affects other orthographic systems such as Chinese and English. In addition, investigation of the relationship between the representation for orthographic (i.e., grapheme or syllable) and nonorthographic systems (i.e., object) will provide additional information for the underlying mechanism of such representation in AD. Lastly, future studies are warranted to explore the specific brain regions related to the orthographic knowledge of Hangul.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
References
Appendix
Appendix 1. The stimuli of the Hangul writing to dictation task

Appendix 2. The stimuli of the Hangul representation task: yes-no questionnaire

Appendix 3. The stimuli of the Hangul representation task: multiple choice test items
