고기능 및 저기능 자폐성장애와 지적장애 아동의 어휘 특성 비교
Vocabulary Characteristics of Children with High and Low Functioning Autism and Intellectual Disabilities
Article information
Abstract
배경 및 목적:
비장애 아동의 경우 표현 가능한 어휘보다 수용 어휘가 높은 것에 비해, 자폐성 아동의 경우 공식검사 결과에서 수용어휘 결과가 낮게 보고 되고 있다. 새로운 낱말을 실제 사물과 연결시킬 때, 자폐성 장애 아동은 다른 비장애 아동과 같이 상호배타성의 원리를 활용할 수 있지만 사회성 결함으로 인하여, 낱말 연결에서 상대방이 제공하는 강화를 적절하게 수용하지 못할 가능성이 있다. 본 연구는 자폐성장애 아동과 지적장애를 동반한 자폐성장애 아동, 그리고 지적장애 아동의 세 그룹 간 표현 및 수용어휘 능력의 차이를 알아보고, 각 그룹에서 보이는 표현 및 수용언어 능력의 차이가 그룹 간에도 유의한 차이를 보이는지를 밝히고자 한다.
방법:
연구에는 10명의 고기능 자폐성 아동과 11명의 지적장애를 동반한 자폐성 아동, 그리고 12명의 지적장애 아동이 참여하였고, 이들의 수용 및 표현어휘 검사를 실시하였다.
결과:
수용 및 표현어휘 점수는 세 그룹 간 유의미한 차이를 보였다. 하지만 각 그룹 내에서 표현 및 수용어휘의 격차는 통계적으로 유의미하지는 않았지만, 자폐성 아동에게 보이는 표현어휘 우세 양상이 고기능 자폐성 아동 집단과 지적장애를 동반한 자폐성 아동 집단에서 일정하게 나타나는 경향을 보였다. 결과에 대한 논의 및 연구의 제한점, 그리고 후속 연구에서 고려할 사항에 대하여 제시하였다.
논의 및 결론:
세 집단의 어휘 능력 간 보이는 경향성은 지적장애 그룹의 상호배타성 원리 사용 가능성을 보여준다. 후속 연구에서는 대상자 수를 늘리고 어휘능력 평가 도구를 보완하는 것이 필요하겠다.
Trans Abstract
Objectives:
Children with autism spectrum disorders (ASD) shows atypicality in various domains in language. One of atypical characteristics in their language can be found in vocabulary. Usually children show greater receptive than expressive vocabularies, but for ASD children the opposite results are reported. Even though children with autism show mutual exclusivity when mapping new words to the correct objects, their social deficits prohibit them from being reinforced by others’ feedback. Thus they can have more difficulty in receiving initiation and directions from others, and as a result, can demonstrate atypical vocabulary characteristics. The purpose of this study is to find out the differences in expressive and receptive vocabulary abilities among children with high functioning ASD, low functioning ASD, and intellectual disabilities (ID), and the discrepancies in expressive and receptive vocabulary among the three groups.
Methods:
Ten high functioning ASD, 11 low functioning ASD, and 12 ID children were tested with the receptive and expressive vocabularies test (REVT).
Results:
The results indicate significant differences in receptive and expressive vocabularies. However, there was no significance between receptive and expressive vocabulary among three groups even though trends of higher expressive vocabularies over receptive can be found in the high and low functioning ASD group.
Conclusion:
The trends of higher expressive vocabulary in the two ASD groups compare to ID group tells high possibilities that children with ID can be reinforced by the feedback that the interaction partner gives. For the future studies, it is necessary to increase the sample size and add assessment tools which can prove vocabulary abilities.
Children with autism spectrum disorders (ASD) range from those who have no verbal language ability to those who can converse with others with varying degrees competence. However, regardless of their speech and language abilities they cannot properly use their knowledge for the purpose of relationships. Even though they may have better vocabulary and grammar knowledge than their peers, they have difficulty in reciprocal conversation (Bedford et al., 2013).
Numerous studies have found that children with ASD have relatively higher ability in expressive language than receptive language, as opposed to typically developing children. The receptive language of typical children advances their expressive language (Kover, McDuffie, Hagerman, & Abbeduto, 2013). Generally, people can understand more than they can speak.
There have been consistent research results about the atypical characteristics in receptive and expressive language ability in children with ASD. Weismer et al. (2011) found that toddlers with autism from ages 24 to 36 months have significantly higher age-equivalent scores in expressive language than receptive language. In contrast, Volden et al. (2011) found that a comparison group of toddlers with developmental delay without ASD displayed the opposite trend. Also, they confirmed the strength of expressive language over receptive language in a large sample of 2- to 4-year-old children with ASD. Seol et al. (in press) reported significantly lower scores in receptive language in ASD children compared to developmental language delayed (DLD) children aged between 20 months to 50 months. According to the researchers, the ASD group was an expressive-language dominant group, compared to the DLD group, which was a receptive-language dominant group. A relative weakness in receptive language abilities is also prevalent in preschool and school-age children with ASD. Loucas et al. (2008) have compared receptive and expressive language abilities between school-aged children with specific language impairment (SLI) and ASD. They found that receptive language was less impaired than expressive language in children with SLI, whereas children with ASD lacked a receptive language advantage. Hudry et al. (2010) found that preschool children with ASD have notably lower scores in receptive vocabulary. Charman, Drew, Baird, & Baird (2003) observed that a sample of 134 preschool children with ASD had an overall delay in vocabulary, with receptive vocabulary being impaired to a greater extent than expressive vocabulary.
Many reports have indicated an atypical relationship between language comprehension and production in children with ASD. However, the extent to which this relationship extends to all individuals with ASD is unclear. Some of these inconsistent results are reported in school-age children with ASD and in their vocabulary ability. Kjelgaard & Tager-Flusberg (2001) examined the language ability of 89 children with autism, of which 44 performed the Clinical Evaluation of Language Fundamentals (CELF; Semel, Wiig, & Secord, 1995) and a vocabulary test. These 44 children got higher scores than control group in the expressive language scores of the CELF but not the vocabulary test. It has been argued that children with ASD are more impaired in receptive language ability (Hudry et al., 2010), but one study showed that approximately 30% of the children with ASD had an atypical pattern of both receptive and expressive vocabulary on the MacArthur Communicative Development Inventories (MCDI; Fenson et al., 1993).
Then, how can we explain the relative weakness of children with ASD in receptive language? One possible theory can come from the mutual exclusivity (ME) principle in typical development of vocabulary acquisition. The ME principle refers to the assumption that novel words refer to unfamiliar objects or objects for which the child does not yet have a label (Bedford et al., 2013). Most parents and caregivers give ostensive and referential cues to young language learners with repetitive labeling of the name of the object. Word learning is subsequently demonstrated in the absence of such cues, in which case infants make use of various heuristics to infer a speaker’s referent, which is ME, and most children start to use this principle toward the end of their second year of life (Halberda, 2003). With or without ostensive and referential cues, whenever labeling happens and a child can associate an object with a word just heard, this kind of word learning context is called fast mapping. In addition, word retention tests following fast mapping show that more context helps children remember newly acquired words; this reinforcement of from the interaction partner, is called feedback (Horst & Samuelson, 2008).
Children with ASD are less responsive to social cues, in particular to referential cues, and some experimental studies have shown that they have difficulties in using cues for word learning. Bedford et al. (2013) studied the ability to use ME and retention of new words in 2-year-old children at risk of ASD. They found that the ME and fast mapping of children with ASD was intact (de Mrchena, Eigsti, Worek, Ono, & Snedeker, 2011) but that they showed differences when using feedback from interaction partners. Language delay in ASD children, especially in vocabulary, could be caused by their lower sensitivity to social-communicative cues; they do not benefit from ostensive feedback and therefore are less able to retain the results of word-object mapping (Baron-Cohen, Baldwin, & Crowson, 1997).
Language is also one of the most impaired areas of children with intellectual disabilities (ID). Studies indicate that children with ID often exhibit poorer language skills compared with typically developing (TD) children of the same mental age (Owens, 2010). The overall sequence of their development is similar to that of TD children before they use words, but their rate of development is slower. They develop intentions, role taking, and presupposition. Chapman, Bird, & Schwartz (1990) studied novel word learning in children with Down syndrome and chromosomal disorders and found out they are as skilled as their mental-age-matched TD peers in inferring novel word meanings and in producing these words correctly thereafter.
There have been mostly consistent research results about the characteristics of vocabulary of children with ASD and ID. Receptive vocabulary is greater than productive (i.e., expressive) vocabulary for typically developing children and conversely (that is, productive > receptive vocabulary) for atypically developing children (Hudray et al., 2010). Expressive vocabulary is less impaired than receptive in ASD children, but there is little research regarding receptive and expressive vocabulary for children with ID. Moreover, many research studies have been done using vocabulary tests from parents’ reports, which mostly compared ASD children with typically developing or language impaired (LI) children. In addition to comparison with typical and LI children, it is necessary to compare the atypical relationship in vocabulary among children with high and low functioning ASD, and ID children in clinical practice. The aim of this study is to find (1) the differences in expressive and receptive vocabulary abilities among children with high and low functioning ASD and ID children and (2) the differences between expressive and receptive vocabulary among three groups.
METHODS
Participants
The participants were 33 children between the ages of 60 months and 94 months who visited a child and adolescent psychiatry clinic. They were divided into three groups: high functioning ASD (HF ASD), low functioning ASD (LF ASD), and ID. Children with ASD and ID were diagnosed by a child and adolescent psychiatrist, using the criteria of the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text-revised (DSM-IV-TR). There are no available diagnostic guidelines for HF ASD and LF ASD. These are the most commonly used clinical descriptors to differentiate individuals with autism. Conventionally, if a child is diagnosed with ASD meeting the conditions of DSM-IV or -5, but displays cognitive ability in the low average to above average range, he or she is said to have HF ASD (Sansosti, Powell-Smith, & Cowan, 2010). In this study, low functioning autism children were diagnosed by the results of cognitive evaluation using the Korean Wechsler Preschool & Primary Scale of Intelligence (K-WIPPSI) and Korean Educational Development Institute Wechsler Intelligence Scale for Children (KEDI-WISC). Data from 55 children (16 children with HF ASD, 22 children with LF ASD, and 17 children with ID) was collected in the beginning of the present study, however, subsequently some children were excluded when they did not meet the criteria of Intelligence Quotients (IQ)—IQ under 40 and borderline IQ between 70 to 80. Vocabulary test scores are meaningless when IQ is too low and standard deviations are too large when borderline intellectual functioning children are included. After these exclusions, there were 10 children in the HF ASD group (9 boys and 1 girl), 11 children in the LF ASD group (8 boys and 3 girls), and 12 children in the ID group (8 boys and 4 girls). Group means and standard deviations for the chronological age of the children and their Verbal Intelligence Quotient (VIQ) and Performance Intelligence Quotient (PIQ) can be seen in Table 1. Mean ages were 76.70 months (range, 63-94 months) for the HF ASD group, 70 months (ranged, 61-87 months) for the LF ASD group, and 73.33 months (range, 60-90 months) for the ID group. Children with HF ASD had a 97.90 mean VIQ score (range, 82-139) and 102.50 mean PIQ score (range 90-134). The LF ASD group had a 67.18 mean VIQ score (range, 53-82) and 60.73 mean PIQ score (range, 49-66). The mean VIQ and PIQ scores of children with ID were 69.17 (range, 53-84) and 65.92 (range, 52-88), respectively. One-way repeated ANOVA was run to compare these characteristics across the three groups. Group comparisons revealed the following: (1) there was no significant difference in chronological age among the three groups and (2) both VIQ and PIQ in the HF ASD group were significantly higher than in the LF ASD and ID group (VIQ: F(2,30)=18.00, p<.001; PIQ: F(2,30)=45.65, p<.001).
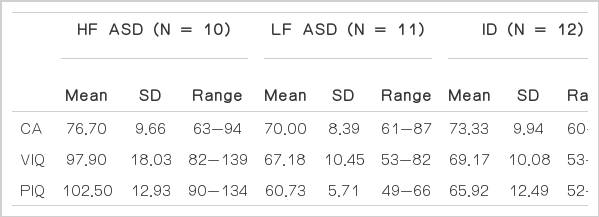
Participants by group, age, VIQ, and PIQ
Language assessment
The receptive and expressive vocabulary test (REVT; Kim, Hong, Kim, Jang, & Lee, 2009), which is standardized Korean vocabulary test, was used in this study. The test consists of a receptive vocabulary test (REVT-R) and an expressive vocabulary test (REVT-E). The item sets are arranged in order of increasing difficulty based on Item Response Theory (IRT). In REVT-R, children are requested to point the appropriate picture among 4 choices; children are requested to name a picture as an examiner shows in REVT-E. The test is suitable for people ranging in age from 2 years old to over 16 years old. In the present study, data was comparing receptive and expressive vocabulary scores from age-equivalent children from other research studies (Abbeduto et al., 2001; Chapman, 2006; Krantz & McClannahan, 1993; Miyamoto, Houston, Kirk, Perdew, & Svirsky, 2003).
RESULTS
Group differences on scores of receptive and expressive vocabulary test
One-way repeated measures ANOVA was performed to compare age-equivalent scores on both the receptive and expressive vocabulary test (REVT) for the three participant groups. The between-subjects effect indicates that group differences were significant (F(1,30)=384.55, p<.001), but the within-subjects effect and interaction effect (REVT by Group) were not statistically different (F(1,30)=231.43, p>.05 and F(2,30)=111.29, p>.05; respectively).
Additionally, MANOVA was used to compare groups with age-equivalent REVT scores and the LSD post-hoc test was conducted to make pairwise comparisons between two of the three groups with REVT scores. As can be seen in Table 2, performances on the receptive vocabulary of REVT was significantly different among the three groups (HF ASD, LF ASD, and ID) in terms of age-equivalent scores (F=13.68, p<.001). LSD post-hoc comparisons revealed significant difference between the HF ASD and the both LF ASD (p<.001) and ID groups (p=.002), but only slightly different between the HF ASD, LF ASD, and ID groups (p=.066). Also, age-equivalent scores (F=11.01, p<.001) on the expressive vocabulary of REVT were significantly different among the three groups. Posthoc tests showed children with HF ASD had consistently higher age-equivalent scores on the expressive vocabulary than the 2 other groups, which did not differ from each other.

Results of post-hoc LSD tests by group for RV AE and EV AE
Comparison of the gap between mean scores of receptive and expressive vocabulary among the groups
Relative receptive and expressive vocabulary abilities for the three groups (HF ASD, LF ASD, and ID) were compared using mean age-equivalent REVT scores as can be seen in Table 2. Figure 1 shows that the score of age-equivalent expressive vocabulary (EV AE) is higher than the score of age-equivalent receptive vocabulary (RV AE) for the HF ASD and LF ASD groups. However, the score of EV AE is lower than the score of RV AE for children with ID.

Receptive and expressive vocabulary trends. HF ASD=high functioning autism spectrum disorder; LF ASD=low functioning autism spectrum disorder; ID=intellectual disability.
CONCLUSION
Receptive and expressive vocabulary abilities were examined through REVT to compare among the groups: children with HF ASD, LF ASD, and ID. The groups showed significant differences in their vocabulary (Table 2). The ID group showed typical characteristics of higher receptive vocabulary ability over expressive ability. The vocabulary characteristics of the LF ASD group were quite the opposite; even though the ID group who had similar intellectual function. This is consistent with previous research even though there can be differences in the experimental and control groups and the tools or domains that are tested (Kover et al., 2013; Seol et al., in press; Volden et al., 2011; Weismer et al., 2011). However, there was no significant difference between receptive and expressive vocabulary among the groups, even though trends of higher expressive vocabulary in the two ASD groups were found.
As the studies with ID children showed, these children can use the ME principle when they hear a new word, similar to children with ASD (Chapman et al., 1990). Moreover, they can develop communicative interactions as TD children do, even though their vocabulary growth is slow (Owens, 2010). This indicates that the vocabulary of children with ID can be reinforced by the feedback that interaction partners give whenever they try to connect new words and objects. Therefore, children with ID show typical receptive and expressive patterns whereas ASD children do not (Figure 1).
As previous studies have shown children with ASD had relatively high scores in expressive vocabulary, but this was not fully supported statistically. This could be explained in some part by the inconsistent results between assessment tools (Hudry et al., 2010; Semel et al., 1995). Furthermore, it can also be noted that the standard deviation of expressive vocabulary in the HF ASD group was substantially higher than receptive vocabulary in the other two groups. The same characteristics were found in the LF ASD group. Inconsistency between assessment tools needed to be examined carefully; however, we must recognize the spectrum of ASDs just as is done in its diagnostic criteria. Such diversity cannot be proved statistically, but definite differences can be seen in the atypicality of receptive and expressive language abilities, not just vocabularies. These results can be explained by the weakness in social reciprocity: children with ASD do not respond to others’ social expressions like imitation, nor model or correct as much as children without ASD do. Therefore, they can express what they see more easily than pointing out what they hear, the latter of which places more of a burden on social reciprocity.
Even though there are group differences in vocabulary abilities and receptive and expressive gaps, there can be limitations from the sample size of this study. Because of the small sample size, it is not easy to generalize the results. If it is possible to analyze similar characteristics with a larger sample size, we may be able to find out whether there are some trends by age or not. The ASD group show ed atypical trends depending on their age or language abilities, while there was no such indication of those trends in the ID group (Table 2).
Furthermore, the results from the REVT were not enough to be fully representative of vocabulary ability. As Bedford et al. (2013) suggests, experimental tasks or semi-structured interactions should be used complementarily. It can be assumed that the group differences in vocabulary abilities come from some underlying basis, when really they are just accidental differences. Also, REVT is a formal evaluation tool which has manuals to follow, which means that children who have good social responses can perform at a higher level. This procedure does not reflect how children make use of their vocabulary in a natural environment. For future studies, it is necessary to increase the sample size. Standardized tests, such as the REVT, are useful in comparing children’s vocabulary ability to their chronological age peers, but research regarding other vocabulary characteristics (such as speech accuracy or rates of error type occurrences), need to be implemented as well.