Huneety, Al-omari, Mashaqba, and Abu Guba: 요르단 아랍어권 말소리장애 아동의 음운능력 평가
초록
배경 및 목적
본 연구는 평균음운길이(PMLU), 단어단위근접률(PWP), 단어단위정확률(PWC), 자음정확도(PCC)가 요르단 아랍어의 음운발달 평가지표로 타당한지 알아보기 위해, 해당 언어를 사용하는 말소리장애 아동과 일반 아동의 자발화 샘플에서 PMLU, PWP, PWC, PCC를 분석하였다.
방법
요르단 아랍어를 단일언어로 사용하는 5세 말소리장애 아동 44명, 일반 아동 44명, 총 88명이 본 연구에 참여하였다. 보호자들과의 놀이상황에서 자발화를 수집하였고, 이 중 100 발화를 말소리 지표 분석을 위해 사용하였다.
결과
말소리장애 아동은 일반 아동보다 모든 지표에서 점수가 유의하게 낮았고, 각 지표값 간에는 유의한 정적 상관관계가 있었다. 말소리장애 집단에서는 조음운동의 어려움을 시사하는 특정 말소리 오류들과 음운오류패턴이 관찰되었다.
논의 및 결론
본 연구를 통해 요르단 아랍어권 말소리장애 아동의 음운발달을 정확하게 진단하고 진전과정을 추적하는 데에 PMLU, PWP, PWC, PCC가 모두 유용한 지표임을 알 수 있었다.
Keywords: 평가 도구, 음운발달, 음운장애, 말소리장애, 일반 아동
Abstract
Objectives
This study investigated the validity of four language measures, i.e., phonological mean length of utterance (PMLU), the proportion of whole-word proximity (PWP), the proportion of whole-word correctness (PWC), and percentage of correct consonants, in assessing phonological development in Jordanian Arabic (JA) speaking children with phonological disorders in comparison with typically developing (TD) children.
Methods
The study involved 88 monolingual JA-speaking children within the age range of 5 to 6 years, with 44 children diagnosed with phonological disorders and 44 TD children. Each group was further categorized into two age groups, namely 5;0-5;6 and 5,7-6,0. Data were gathered by observing the interactions between the children and their caregivers or parents using age-appropriate toys. A minimum of 100 utterances were collected from each participant.
Results
The study found that TD children performed better than the children with phonological disorders on all measures, indicating delayed phonological performance in the phonological disorders group. Positive correlations between the measures were also observed, indicating their ability to provide significant information about children’s phonological abilities. Specific speech sound errors and substitution patterns exhibited by children with phonological disorders were identified, highlighting the motor control and articulatory challenges experienced by this group. Age was found to be a significant factor in the development of TD children, while children with phonological disorders showed similar scores across different age groups.
Conclusion
These findings support the usage of the four measures for understanding phonological development in children with phonological disorders, accurately diagnosing them and tracking their progress.
Keywords: Assessment tools, Phonological development, Phonological disorders, Speech sound disorders (SSD), Typically developing (TD) children
A substantial amount of literature on Arabic has been dedicated to evaluating child language through articulation tests, with a primary focus on assessing the accuracy of segmental productions ( Amayreh & Dyson, 1998; Amayreh & Dyson, 2000; Hamdan & Amayreh, 2007; Mashaqba et al., 2019; Mashaqba, Daoud, Zuraiq, & Huneety, 2022), or through acoustic tests focusing on the formant frequencies and vowel space area ( Mashaqba, Huneety, Al-Khawaldeh, Al-Deaibes, & Zeidan, 2023). Recently, research has shifted focus from articulation tests to word complexity and utterance length ( Burrows & Goldstein, 2010; Ingram & Ingram, 2001). For instance, several studies, Ingram and Ingram (2001); Taelman, Durieux, and Gillis (2005); Kumar and Bhat (2009); Huneety, Khashashneh, Mashaqba, Guba, and Alshdaifat (2023), described the phonological development of typically developing (TD) and distinguished them from impaired children through whole-word measures. The whole-word model assesses children’s ability to accurately produce complex words, providing valuable information into their phonological development ( Burrows & Goldstein, 2010). The concept of whole-word measures, originally proposed by Ingram and Ingram (2001), involves analyzing words as a whole, taking into account factors such as correctness, complexity, and variability ( Ingram & Ingram, 2001). This model, which is based on the accurate production of segments, has gained broad acceptance in clinical practice due to its direct approach in measuring children’s phonological skills and its ability to differentiate TD children from those with impaired development. One commonly used whole-word measure is the phonological mean length of utterance (PMLU), which indicates the complexity of the child’s productions. In addition to the PMLU, several measures are used, including the proportion of whole-word proximity (PWP), and the proportion of whole-word correctness (PWC). These measures provide rich information for assessing word complexity and production accuracy at the level of word production and in conversational speech. For further details on these measures, please refer to Section 1.2.
Despite all research efforts to understand phonetic and phonological behaviors of children with language impairment in other languages ( Holm & Dodd, 1999; Yavaş & McLeod, 2010; Zhu & Dodd, 2000; Farquharson, Hogan, & Bernthal, 2014), there is still a literature gap focusing on Jordanian Arabic (JA) children with phonological disorders, whose native language, Arabic, is one of the most widely spoken languages in the world. Available standardized tests on English-speaking children may not be adequate for assessing Arabic-speaking children due to the unique phonetic and phonological features of Arabic and the distinct phonological systems of these two languages. Moreover, the growing body of research on JA-speaking children has primarily centered on how TD children acquire their native language, where there is no single study addressing the phonology of JA-speaking children with language impairment. This accentuates the importance of scrutinizing the phonological performance of JA-speaking children with phonological disorders to better explore their phonological challenges and develop practical strategies of therapeutic intervention. The present study seeks to fill the gap in literature and introduce a novel tool for evaluating the phonological skills of JA-speaking children aged 5-6 years with phonological disorders, utilizing both lexical and segmental measures. We hypothesize that both types of measures are useful tools for speech pathologists to evaluate children’s phonological abilities and to identify those with atypical phonological development ( Gerrits & de Bree, 2009; Kumar & Bhat, 2009). Employing these measures allows speech pathologists to promptly provide children with phonological disorders with the necessary and suitable rehabilitation services.1 The present work targets children within the age group of 5-6 years, intending to investigate a critical period in children’s phonological development. This age period is considered a decisive stage in language acquisition, where children typically experience significant progress in their phonological and articulatory skills. Previous research suggests that the age range of 5-6 years old is characterized by substantial variability in language development, making it an appropriate time to explore differences in phonological abilities ( Mashaqba et al., 2021). More specifically, focusing on this age group enables us to capture a crucial stage before formal schooling begins, providing insights into early phonological challenges that may impact a child’s readiness for literacy development ( Mashaqba et al., 2022. This study is a follow-up to Huneety et al.’s (in press), who proved the efficiency of the four measures in reflecting the phonological development of children and recommended conducting another study to check the usage of these measures to distinguish TD children from children with language impairments. The primary rationale for employing the four measures was to ensure the comprehensiveness and efficacy of our assessment, providing speech pathologists with a holistic understanding of children’s phonological development. Each measure captures distinct aspects, including phonological complexity, word production, and overall speech accuracy (cf. section 5). Moreover, languages can exhibit unique features and complexities, and the interactions among these measures may vary ( Saaristo-Helin et al., 2006; Taelman et al., 2005).
Literature Review
The following literature review provides an overview of relevant studies on phonological abilities using whole-word measures in three distinct groups: monolinguals, bilinguals, and children with language impairments. This will be followed by a discussion of related studies specifically focusing on the context of JASC.
Several cross-linguistic studies have examined the phonological abilities of monolingual children using whole-word measures, particularly PMLU, reflecting phonological and morphological development ( Gerrits & de Bree, 2009; Ingram, 2002; Kumar & Bhat, 2009; Saaristo-Helin et al., 2006; Taelman et al., 2005). Ingram (2002) categorized the PMLU scores of English-speaking children into five stages, which correlated with their age. Taelman et al. (2005) collected longitudinal data from Dutch-speaking children and found that PMLU scores correlated with age with an average increase of 0.18 points per month. Beers, Rodenburg-Van Wee, and Gerrits (2019) conducted a study on Dutch-speaking children and found a significant increase in PMLU scores over age with the most noticeable growth occurring in the age group between 1;3 and 1;11. Burrows and Goldstein (2010) investigated whole-word measures in Spanish-English bilingual children who had phonological disorders. The study found that monolingual children had higher PCC, PMLU, and PWP scores compared to bilingual children. However, the study supported the use of PMLU, PWP, and PCC as measures to assess the phonological abilities of both monolingual and bilingual children with speech sound disorders (SSDs), as significant correlations were found between these three measures.
Several studies have compared whole-word measures between TD children and children with language impairment ( Gerrits & de Bree, 2009; Kumar & Bhat, 2009). Gerrits and de Bree (2009) examined PMLU and PCC measures in Dutch-speaking threeyear-old children and found that TD children had higher PMLU and PCC scores compared to children with a familial risk of dyslexia and children with specific language impairment (SLI). Similarly, Kumar and Bhat (2009) found significant differences in PMLU scores between TD Kannada-speaking children and children with phonological disorders, advocating the use of PMLU as a diagnostic tool for identifying children with phonological disorders. Saaristo-Helin (2011) demonstrated that whole-word measures are very suitable for children with SLI struggling with the production of multisyllabic words. This approach efficiently captures any improvement in children’s performance, unlike the segmental method, which may not adequately capture the progress made by children. Only one study has been conducted on TD JA-speaking children, namely Huneety et al. (in progress). This study examined four whole-word measures (i.e., PMLU, PWP, PCC, and PWC) in TD children. The data were collected from a total of 30 participants, divided into three age groups: 1;7-2;0, 2;1-2;6, and 2;7-3;0 years. The study introduced a novel adjustment called the “gemination rule” for calculating PMLU in Arabic. According to this rule, two points were assigned for producing the geminate correctly, and two additional points for the accuracy of the geminate. The results of the study indicated that these four measures effectively captured the phonological development of children across all three age groups. It found significant correlations between PMLU, PWP, and PCC measures, while no significant correlation was found for the PWC measure.
As can be seen, whole-word measures have been utilized to evaluate the phonological development of TD monolingual, bilingual, and children with language impairment to identify any deviations in their development. Understanding the phonological abilities of these children and the challenges they face can help inform the development of effective interventions that promote successful communication and language development. However, there is a gap in the literature regarding the use of these measures in JAspeaking Arabic with phonological disorders. This research aims to address this gap and assist speech-language pathologists (SLPs) in accurately determining a child’s developmental stage and identifying an SSD. Consequently, the primary objectives of this study are to investigate whether there are differences in the overall scores of these four measures (i.e., PMLU, PWP, PWC, and PCC) between TD children and children with phonological disorders, and whether child age affects his/her performance in both groups. Additionally, the study aims to find if there is any correlation between these measures within both TD children and children with phonological disorders. The study hypothesizes that:
Hypothesis (1): TD children will exhibit significantly higher average scores in PMLU, PWP, PWC, and PCC compared to children with phonological disorders in both age groups:
We hypothesize that TD children will demonstrate superior performance across measures (PMLU, PWP, PWC, and PCC) compared to children with phonological disorders in both age groups. This expectation is grounded in existing literature ( Gerrits & de Bree, 2009; Kumar & Bhat, 2009) indicating that TD children generally exhibit more developed articulation and phonological skills. Hypothesis (2): There is a significant main effect of child age group on the performance of TD children in the four measures but not for the phonological disorders group:
Our second hypothesis posits that there will be a noteworthy main effect of a child age group on the performance of TD children across the four measures (PMLU, PWP, PWC, and PCC). This is based on the widely acknowledged principle that linguistic development in TD children is influenced by age. In contrast, we anticipate that such age-related effects may not be as pronounced in the group with phonological disorders due to potential variations in developmental trajectories.
Hypothesis (3): There is a significant correlation between PMLU, PWP, PCC, and PWC within the two groups:
The third hypothesis proposes a significant correlation between PMLU, PWP, PCC, and PWC within both the TD children and phonological disorders groups. This hypothesis stems from the assumption that these measures, focusing on articulation and phonological aspects, are interconnected and reflective of overall language development. A strong correlation within each group would suggest a consistent pattern in the participants’ linguistic performance across these measures.
Hypothesis (4): Children with phonological disorders exhibit a set of universal error types in their speech, suggesting common underlying patterns indicative of the disorder.
METHODS
Participants
The study included a total of 88 monolingual JA-speaking children between the ages of 5 and 6 years. All participants were native speakers of Ammani Arabic and resided in Amman. The participants were divided into two groups: 44 children diagnosed with phonological disorders who belonged to two age groups (group I included 22 children 5;0-5;6 years (mean age 5.3) and group II comprised 22 children aged 5,7-6,0 years (mean age 5.8). A SLP assessed all the participants to confirm the diagnoses of those with phonological disorders and to make sure that TD children had neither communication nor hearing disorders. The TD children were selected from three nurseries in Amman and were divided into two age groups i.e., 22 children aged 5;0-5;6 years (mean age=5.28) and another 22 children aged 5;7-6;0 years (mean age=5.75).
Data Collection
The data collection process extended over a period of three months, with each child engaging in three sessions that lasted between 25 and 30 minutes per session. The data were collected by observing the interactions between the children and their caregivers or parents during free play. Age-appropriate toys and activities were incorporated to facilitate data collection. Additionally, each child was presented with 15 colorful pictures featuring different word shapes to encourage speech production. Some children were provided with cues to assist them in producing the target words. The researchers made sure that a minimum of 100 utterances were obtained from each child.
To capture the speech samples, an iZYREC Digital Voice Recorder was utilized. The recorder was positioned approximately 6-8 inches away from the child’s mouth to ensure clear audio recordings. All recorded files were securely saved on a Toshiba laptop to prevent any loss of data.
Procedures and Data Analysis
During the data analysis phase, the lexical-size rule ( Ingram & Ingram, 2001) recommended a minimum sample size of 25 words, preferably 50 words. However, in this study, a sample of 50 words was randomly selected from each child after excluding nonsense words, onomatopoeic words, fillers, repetitions, and interjections. This was done to ensure that the data collected were representative and included different word shapes such as monosyllabic, disyllabic, and multisyllabic words. Following the variability rule proposed by Ingram and Ingram (2001), when multiple forms of the same word are produced, the most frequent form is considered. For example, if the word /til.fiz. jo:n/ ’television’ has three different forms produced by the participant as [zi.jo:n], [fizjo:n], and [jo:n], the form with the highest frequency (in this case, the second form) is counted. The selected sample was analyzed using the following measures: PMLU, PWP, PCC, and PWC, based on the rules proposed by Ingram and Ingram (2001) and adapted by Huneety et al. (in progress) for calculating whole-word measures in Arabic. These rules can be summarized as follows:
a) The production rule and consonant correct rules are used to calculate the child’s PMLU scores. Each segment of the word is awarded one point, and an additional point is given for each correct consonant. For example, the word milḥ ‘salt’ has a target PMLU score of seven points, four points for the four segments (/m/, /i/, /l/, and /ḥ/), and three points for the three correct consonants (/m/, /l/, and /ḥ/). If the child produces this word as [miḥ], the child’s PMLU score would be five, three points for the length of the segments and two points for the correctness of the consonant. However, added segments are not given any points to avoid situations where the child’s form has a higher score than the target word. Consonant distortions, substitutions, and omissions are considered errors as children aged 5-6 years are expected to have acquired all consonants. b) Huneety et al. (in progress) proposed two additional rules to complement the existing ones: the positional rule, based on Bónová, Slancová, and Mikulajová (2005), and the gemination rule. The positional rule considers metathesis, which involves rearranging segments within a word, and it states that a segment is deemed correct when it aligns with the actual word’s position. The gemination rule treats geminates (consecutive identical consonants) as two separate consonants. Thus, two points are assigned for the preservation and correctness of the geminate. For example, in the word sabbaḥ ‘to help someone swim’, two points are awarded for the geminate and two points for its correctness. If a child mispronounces the geminate but preserves its length (e.g., “bal.la” instead of “bar.ra” for ‘outside’), one point is given for each occurrence of the geminate because geminates are contrastive units in Arabic and help in deducing the meaning of the word even when mispronounced (Abu Guba, 2021; Mashaqba et al., 2021). Moreover, if the geminate is produced as a singleton (e.g., [qadar] for qaddar ‘to estimate’, one point is awarded for the singleton and another point for the correctness of the consonant). Based on these rules, the PWP, PCC, and PWC scores for each word were computed. c) To calculate the PWP, the child’s PMLU mean is divided by the mean target PMLU score (child’s PMLU score÷target PMLU score=PWP). For example, the PWP score for the word fa:ḥ ‘apple’ (PMLU=5) from tuf.fa:ḥ (target PMLU=10) 0.5 or 50%. d) To calculate the PWC measure, a correct form without errors is assigned one point, while an incorrect form receives zero points. For instance, if a child produces 60 words correctly out of 100, the PWC would be 60%. e) The PCC is calculated by giving one score for each correctly produced consonant, while an incorrect consonant receives a score of zero. The total number of correct consonants is then divided by the total number of consonants to determine the percentage of correct consonants. If the child, for example, produces 40 correct consonants out of a total of 200 consonants, the PCC score would be 0.2 (20%).
To test the research hypotheses, we submitted the collected data to statistical analysis using open access language R, version 4.3.0, and utilizing five R packages: tidyverse ( Wickham et al., 2019), ggpubr ( Kassambara, 2023a), rstatix ( Kassambara, 2023b), car ( Fox & Weisbergm, 2019) and broom ( Larmarange & Sjoberg, 2023).
Transcription and Reliability
The speech samples were manually transcribed by two experienced SLPs because they have experience in working with children with phonological disorders. In addition to transcription, they provided glosses for the children’s productions, indicating the phonological processes involved, to ensure clarity of reference. To ensure transcription reliability, 25% of the recorded data was independently transcribed by two blind transcribers. The overall percentage agreement between the transcriptions was 93.9%. Any discrepancies between the two transcriptions were resolved through discussion, resulting in a final agreement of 100%.
RESULTS
Figures 1- 4 and Table 1 compare children’s mean scores of PMLU, PWP, PCC, and PWC across their language development (disordered vs. typical) and age group (older vs. younger).
The numerical results show that the TD group outperformed the group with phonological disorders in their responding scores. It is noteworthy that children with typical phonological development showed higher values in PMLU, PWP, PCC, and PWC compared to children with phonological disorders, with increases of 3.70, .33, .37, and .86 points, respectively. Table 1 also suggests a small overall numerical scoring advantage for the typical older children over the typical younger children on the four tested measures: PMLU (mean difference=.44), PWP (mean difference= .026), PCC (mean difference=.027), and PWC (mean difference= .014). To validate the observed pattern of results, a set of multivariate analysis of variances (MANOVAs) were performed.2 Three tests were designed to inferentially determine the possible effect of child language development (disordered vs. typical) and/or child age group (older vs. younger) on the four testing tools: Child PMLU, PWP, PCC and PWC. The cbind() function was used to combine and bundle the four dependent variables together into one weighted composite variable. First, three separate linear regression models were fitted using the lm() function. The first two models were simple models, including either participants’ language development or their age group. The third fitted model included both independent variables, while the fourth model was a full model (i.e., more complex model) testing any possible interaction between participants’ language development and their age group. Each fitted model was computed separately employing the Manova() function of car package and using Pillai’s trace test of multivariate statistics. Then we compared the smaller model to the larger model using the Anova() function at the p<.05 level.
Table 2 shows the results of the final (i.e., the best fitted) MANOVA model. The model identified three significant effects. Firstly, there was a statistically significant difference between children’s language development on the overall combined dependent variables (PMLU, PWP, PCC, and PWC), F(4, 81)=3,935.7, p<.001. Secondly, the model yielded statistically significant differences between child age group on the combined dependent variables, F(4, 81)=3.6, p=.01. Lastly, a significant language development by age group interaction was identified, F(4, 81)=3.3, p<.05. This result suggests that the effect of child language development or child age group depends on the level of the other variable.
To explore the source of the interaction, we performed follow-up pairwise comparisons, adjusted to Bonferroni. Post hoc tests presented in Table 3 show that TD children scored a higher overall mean value compared to children with phonological disorders in both age groups: in the younger child group, F(4, 81)=1,930, p<.001, and in the older child group, F(4, 81)=2,008, p<.001. Additionally, post hoc tests revealed a higher overall mean score for older children relative to younger children with normal language development, F(4, 81)=6.713, p<.001. Children with phonological disorders, on the other hand, showed no significant differences in their overall phonological scores based on their age, F(4, 81)=.122, p=.974. These findings support the first research hypothesis, indicating that children with typical phonological development demonstrate higher scores in PMLU, PWP, PCC, and PWC in comparison to children with phonological disorders. Moreover, these results address the first research question, providing evidence of significant differences in PMLU, PWP, PCC, and PWC between children with phonological typicality and those with phonological disorders. Additionally, the outcomes confirm the second research hypothesis, suggesting that older TD children achieve higher overall phonological scores than younger TD children. However, for children with phonological disorders, the results indicate no significant variations in their overall phonological scores based on age. Thus, these findings address the second research question regarding the impact of age on the scores of TD children and children with phonological disorders.
We followed up the fitted two-way MANOVA with a set of twoway univariate analysis of variances (ANOVAs) to examine, separately, the specific dependent variables that contribute to the significant overall effect. We used the anova_test() function of rstatix package to compute the two-way ANOVAs after considering a Bonferroni adjusted alpha level of .0125. Table 4 shows how the mean of each quantitative variable (i.e., PMLU, PWP, PCC, and PWC) changes according to the levels of the two independent variables: child language development and child age group. When a two-way ANOVA reveals a language development by age group interaction, we intended to carry out Tukey’s post hoc tests for each group of participants by employing the tukey_hsd () function of [rstatix package]. These pairwise comparisons help us explore the source of significant interactions when needed. The first follow-up univariate ANOVA revealed a statistically significant main effect of child language development on PMLU, such that TD children outperformed children with phonological disorders on the mean score of the tested PLMU measure, F(1, 84)= 2,283.833, p<.001. There was a reliable main effect of child age group with a significantly higher mean score of PMLU for older children compared to the younger group of children, F(1, 84)=8.84, p=.004. Finally, the language development by age group interaction was significant, suggesting that the effect of one variable depends on the value of the other variable, F(1, 84)=7.83, p=.006. To determine the direction of the interaction (i.e., which groups are different), we performed post hoc tests separately for child language development and child age groups. The pairwise comparisons, given in Table 5.1., revealed that TD children significantly scored higher average points of PMLU compared to children with phonological disorders in both age groups. Moreover, typical older children reported significantly a higher mean score of the PMLU measure compared to typical younger children, while children with phonological disorders did not report any significant differences on the same PLMU measure based on their age group. The statistical patterns of the PWP and PCC scores were comparable with the PMLU scores. Results yielded significant main effects of child language development, with significantly higher PWP mean scores for typical children compared to children with phonological disorders, PWP: F(1, 84)=5,777.791, p<.001; PCC: F(1, 84)=4,957.272, p<.001. The same ANOVAs revealed reliable main effects of child age group, with higher PWP and PCC average scores achieved by older children compared to younger children, PWP: F(1, 84)=11.14, p=.001; PCC: F(1, 84)=6.30, p=.014. The analysis yielded significant language development by age group interactions for the PWP measure, F(1, 84)=7.84, p=.006, and for the PCC measure, F(1, 84) =7.20, p=.009. To explore the significant two-way interactions, we performed separate post hoc tests for child language development and for child age group. In line with our PMLU analysis above, pairwise comparison tests, summarized in Table 5.2 and 5.3., confirmed that TD children had an advantage of PWP and PCC mean scores over children with phonological disorders regardless of their age group. Results also showed that typical older children outperformed typical younger children on the mean scores of both PWP and PCC measures. However, older and younger children with phonological disorders did not yield statistically significant differences in their PWP and PCC mean scores. The last two-way ANOVA of the PWC measure revealed only a significant main effect for child language development: TD children were more accurate than children with phonological disorders in the PWC measure, F(1, 84)=15,716.760, p<.001, with no significant main effect of child age group, F(1, 84)=1.96, p=.165, nor any significant interaction effect between the two tested variables F(1, 84)=.45, p=.507. Accordingly, the analysis need not to be explored further here.
Results of the four ANOVA tests and the post hoc comparisons discussed above support the research hypothesis that TD children will exhibit significantly higher average scores in PMLU, PWP, PWC, and PCC compared to children with phonological disorders in both age groups. Furthermore, they partially support the hypothesis that there is a significant main effect of child age group on the performance of TD children in PMLU, PWP, PCC, but not for the PWC. However, it was expected that children with phonological disorders will not show any significant differences in the PMLU measure based on their age group.
Table 6 presents the Pearson correlations of PMLU, PWP, PCC, and PWC within each level of child language development. Correlations of the four tested measures were positive and statistically significant within both typical and disordered groups of children. Analysis of the typical group showed a strong correlation between PCC and PWP scores, moderate correlations between PWP scores and both PMLU and PWC scores. There was also a moderate correlation between PWC and PCC scores of the TD child group. Pearson correlations attested a low positive association between the PMLU measure scores and both PCC and PWC measure scores of the TD child group.
Analysis of the group with phonological disorders revealed a moderately strong correlation between PMLU and PCC, moderate correlations between PWP scores, on the one hand, and both PMLU, PPC, and PWC scores, on the other. It also showed relatively weak correlations between PWC measure scores and both PMLU and PCC measure scores of the children with disorders.
These Pearson correlations support the hypothesis that there is a positive and statistically significant relationship between various linguistic measures (PMLU, PWP, PCC, and PWC) within both typical and disordered groups of children.
To summarize, TD children scored significantly higher overall than their peers with phonological disorders, regardless of the age group. However, the scoring difference between TD children and children with phonological disorders was significantly greater in the older age group than in the younger age group. When analyzed individually, the results for each measure were similar except for the PWC measure. While older TD children performed better than the younger TD children in PMLU, PWP, PCC, no significant difference was found between old and younger children with phonological disorders in any of the four tested measures. Finally, children showed some discrepancies in the correlational strength of their tested measures based on their language development. TD children demonstrated a strong association between PCC and PWP, and a moderate correlation between PCC and PMLU; whereases children with phonological disorders showed the opposite correlational match.
The study hypothesizes that children with phonological disorders exhibit a set of universal error types in their speech that lead to low PMLU, PWP, PCC, and PWC scores. After glossing children’s speech production and examining their phonological processes, we found that the most frequent processes that affected the scores of children were de-emphasis, sound substitution and distortions (fronting, stopping of fricatives and affricates, velar fronting), final consonant deletion, cluster reduction, and weak syllable deletion. Table 7 below summarizes the phonological processes performed by the children with some illustrative examples.
DISCUSSION
This study aimed to assess the validity of three whole-word measures (PMLU, PWP, PWC) and a segmental measure (PCC) in reflecting the phonological development of children with phonological disorders and distinguishing them from TD children. The results revealed that TD children significantly outperformed the impaired group in the four tested measures (PLMU, PWP, PWC, and PCC), suggesting delayed phonological performance by the phonologically disordered group. The findings of our study are consistent with previous studies conducted on other languages, showing the validity of the whole-word measures in distinguishing TD children from children with phonological disorders ( Kumar & Bhat, 2009; Gerrits & de Bree, 2009; Saaristo-Helin, 2011). Moreover, the current study demonstrates positive correlations between the four tested language measures in both typical and disordered groups of children. These results suggest that these measures are interrelated and provide complementary information about children’s phonological abilities. For example, although the PCC measure offers valuable information regarding the severity of SSDs ( Shriberg & Kwiatkowski, 1982), unlike PCC, PMLU adequately assesses children’s ability to produce polysyllabic words. We agree with Saaristo-Helin (2011), who claims that PMLU is a more reliable measure for languages like Finnish and Arabic, where long words are common. While PMLU effectively represents the complexity of children’s speech, the PWP can elucidate the differences among children with comparable/similar PMLU values ( Ingram, 2002; Saaristo-Helin, 2011). Additionally, where children with impaired phonology can produce mono- and disyllabic words correctly, it is the PWC measure that shows how many correct words a child can produce. In the literature, difficulty pronouncing multisyllabic words accurately may serve as an indicator of literacy impairment ( Larrivee & Catts, 1999; Huneety, Mashaqba, Al-Shdifat, Khasawneh, & Thnaibat, 2023). Accordingly, incorporating the four measures of phonological assessment provides a more profound understanding of child language disorders. Similar to Kumar and Bhat (2009), the lower PMLU scores observed in children with phonological disorders can be attributed to two main factors: a higher frequency of incorrect consonant usage in their speech compared to TD children, and the utilization of syllable reduction strategies. Bauman-Waengler (2008) demonstrates that children with phonological disorders frequently encounter challenges with different phonemes. Their distorted pronunciations may encompass entire sound classes (for example fricatives). This hinders the child’s ability to establish phonemic contrasts, resulting in the neutralization of phonemic oppositions. Some studies assume that these challenging sounds fall within children’s capabilities, but they fail to use them contrastively to distinguish meaning ( Bauman-Waengler, 2008). That is, children with phonological disorders appear to lack an understanding of the language-specific function and/or organization of certain phonemes ( Fey, 1992; Smith, 1973). Likewise, in the present study, the lower scores of children with phonological disorders compared to TD children may be attributed to the higher rate of incorrect consonant production and simplification processes. First, children with phonological disorders exhibit difficulties in producing consonant sounds, which manifest itself in various ways, including substitutions, omissions, or distortions. For instance, these children may substitute one sound with another due to their inability to accurately produce the target sound. An example of such substitution is observed when a child pronounced the word muf.ta:ḥ as muf.ta:h ‘key’, substituting the pharyngeal /ḥ/ with the glottal /h/ sound, which is easier for them to articulate. This substitution suggests that the precise control required for producing pharyngeal sounds like /ḥ/ poses challenges for children with speech difficulties. Consequently, they resort to substituting it with the glottal /h/ sound, reducing the motor effort needed for articulation. Interestingly, several studies have shown that guttural sounds pose a significant challenge and are considered very problematic for various second language learners ( Eads, Khater, & Mielke, 2018; Mashaqba, Huneety, Abu Guba, & Al-Duneibat, 2022). The production of emphatic sounds (the interdental /ḏ/̣, the dental stop /ḏ/, the alveolar fricative /ṣ/ and the voiceless plosive /ṭ/) proves also challenging for children with phonological disorders. Most children with phonological disorders substitute them with other plain consonants, i.e., mostly /ṭ/ was produced as /t/ or /d/, /d/ as /d/, and /ṣ/ as /s/. Nevertheless, the findings of this study demonstrated that some TD children were able to produce these emphatic consonants in an adult-like fashion, particularly in wordfinal position and in polysyllabic words. The difficulty in producing these consonants can be attributed to two reasons. Firstly, these consonants are among the least frequently occurring consonants in their dialect, resulting in limited exposure and practice. Secondly, emphatics pose challenges due to their articulatory complexity, specifically the involvement of secondary co-articulation known as pharyngealization ( Mashaqba et al., 2022). As children’s articulatory muscles are still developing, they may struggle to achieve the necessary motor control and coordination for these intricate movements. Where children with phonological disorders could not produce emphatics, TD children were able to produce them correctly with an accuracy of 95%. This supports Mashaqba et al. (2022)’s, who found that in Ammani Arabic, there was a delay in the acquisition of emphatic consonants compared to non-emphatic consonants. According to them, over 50% of Ammani Arabic-speaking children produced emphatic consonants by the age of 3, over 75% produced them by the age of 4, and over 90% mastered them by the age of 5. Additionally, children with phonological disorders in this study struggle with sounds produced at the back of the mouth, such as /k/, /g/, /q/, and /ġ/. They tend to substitute these sounds with consonants produced at the front of the mouth, typically /t/ and /d/. For example, the word kaff ‘palm of the hand’ may be produced as taff, and qalb ‘heart’ as dalb. In contrast, only one instance of velar fronting, where velar sounds are substituted with front sounds, was observed in a 5.1-year-old TD child. Previous research by Amayreh and Dyson (2000) has shown that the fronting of velar and uvular sounds is a common pattern among TD children but tends to disappear by the age of 42 months. Alqattan (2015) found that the process of fronting was observed in the youngest age groups (1;4-1;7 and 1;8-1;11) of Kuwaiti-speaking children, occurring in approximately 9% of the attempted target words. In contrast, the oldest age group (3;4-3;7) demonstrated this error in only about 1% of the target words. Velar fronting of vowels has been regarded by Bauman-Waengler (2008) as a marker of children with phonological disorders, such as changing [u] into [i]. Concerning English, Bauman-Waengler (2008) documented the case of Lillian, aged 5.6, where her teacher noted that at times she cannot understand her. Lillian used a number of simplification processes like velar fronting, stopping of fricatives and final consonant deletion, which were markers of phonological disorders. Stopping of fricatives and affricates was also observed in children with phonological disorders, as evidenced by examples such as ša:ḥina and ja:mᶜa which were produced as ta:ḥina ‘lorry’ and da:mᶜa ‘university’ respectively. Dyson and Amayreh (2000) reported that the /k/ and /q/ sounds were occasionally fronted by the youngest children, but this was not observed for the sounds /x/ and /ġ/. However, this specific pattern occurred infrequently, accounting for no more than 7% of the time, and disappeared by the age of 42 months. In certain instances, children with phonological disorders may exhibit final consonant deletion, leading to lower scores in PMLU, PWP, PCC, and PWC measures. For example, in the word madrasa (school), the consonant in the coda position is deleted, resulting in ma.ra.sa. Consonant deletion primarily affects consonants in the coda position due to the obligatory nature of onsets in Arabic syllable structure ( Mashaqba et al., 2019; Watson, 2002). It is worth noting that no instances of coda deletion were reported in the TD group. This pattern tends to be more frequent in younger children below the age of 4. For example, Alqattan (2015) found that coda deletion was a common error pattern in Kuwaiti-Arabic speaking children, particularly prominent in the youngest age groups (1;4-1;7), where 19% of the target consonants were deleted. However, this frequency decreased to 5% in the oldest age group (3;4-3;7). Huneety et al. (2023) demonstrated that even in multisyllabic words, final consonant deletion was observed in only two cases among children aged 3-3;6 and 3;7-4 years old. Reporting on a case of a 3.6-year-old child, Bauman-Waengler (2008) highlighted that typically, final consonant deletion stops by age 3;0, while stopping of [v], [θ], and [ð] persists until age 3;6 or later. Consonant cluster reduction also tends to be suppressed until a relatively late age. Given these findings, the only process that might raise concerns at this age would be final consonant deletion (ibid). Further, children with phonological disorders exhibit cluster reduction in 65 out of the 73-target words. For instance, the words kṯi:r ‘much’ and mba:riḥ ‘yesterday’ were produced by phonologically disordered children as [ti:r] and [ba:rih] respectively. No cases of cluster reduction were attested by TD children. As per Huneety et al. (2023), it was observed that TD JA-speaking children in the age groups of 3-3;6 and 3;7-4 tended to reduce clusters in multisyllabic words. However, no instances of cluster reduction were found in older age groups. Bauman-Waengler (2008) classifies cluster reduction as one of the idiosyncratic features of the speech of children with phonological disorders. Relevant to consonant deletion is the weak syllable deletion, which significantly led to lower PMLU, PWP, PWC, and PCC scores. None of the TD groups applied weak syllable deletion compared to 143 cases of weak syllable deletion by the phonological disordered groups. Out of the 143 cases of weak syllable deletion, only 5 were registered in disyllabic words and the other 138 words were in polysyllabic words. Thus, word shape is an important factor in the diagnosis of children with phonological disorders because a phonologically disordered child may do well in preserving the syllables in mono- and disyllabic words but not in polysyllabic words ( Mashaqba et al., 2019). While TD Jordanian children aged (3-4;6) omitted weak syllables in multisyllabic words, the oldest group (4;7-5) had no cases of weak syllable deletion. In English, Ingram (1989) and Grunwell (1987) provided evidence showing that weak syllable deletion continues to impact children until they reach the age of 4. This phenomenon is related to the position of the syllable. In agreement with Huneety et al. (2023), weak syllables were deleted in initial and medial syllables but never in final positions. Overall, these observations highlight the specific speech sound errors and substitution patterns exhibited by children with phonological disorders. These difficulties are characterized by challenges in producing pharyngeal and emphatic sounds, substituting back-of-the-mouth sounds with front-of-the-mouth sounds, and stopping of fricatives and affricates. While these phonological processes (error patterns) were noticed in the speech of children with phonological disorders, they were only attested in a few cases in the speech of TD children, but are usually found in the speech of younger children (below 4 years old) ( Ingram, 1981). Thus, when unusual phonological errors show up after the age of 4-5, they might indicate delayed phonological development and need clinical intervention. Noteworthy, the speech of children with disordered phonological systems may display differences in the types of phonological processes compared to those with typically developing systems ( Bauman-Waengler, 2008). Thus, phonological processes offer speech pathologists a means of classifying error patterns observed in disordered speech, aiding in the identification of intervention strategies. Nevertheless, it is crucial to exercise caution when interpreting phonological processes as definitive evidence of a phonological disorder (ibid). Although certain error patterns, such as weak syllable deletion and cluster reduction, are universal ( Ayyad, 2011; Bauman-Waengler, 2008; Mashaqba et al., 2019; So & Dodd, 1995), specific errors are language-specific. For instance, in this study, the production of emphatics, gutturals, and geminates poses a challenge to Arabic-speaking children. This accounts for the lower PMLU, PWP, PWC, and PCC scores in Arabic compared to other languages. According to Huneety et al. (in progress), the PCC for TD Arabic children aged 1;7-2 years old was 35.8, increasing to 42.9 for those aged 2;1-2;6, and reaching 49 for children aged 2;7-3 years old. Furthermore, the PWP scores for the same age groups were notably lower, with scores of 56.7 for children aged 1;7-2, 66 for those aged 2;1-2;6, and 70.6 for 2;7-3 years old children. This contrasts with Finnish, where children aged 1;2-2 years had a mean PWP score of 0.78 and PWC of 0.23 ( Saaristo-Helin et al., 2006). The PWC mean score of TD English children aged 0;11 and 1;10 was 0.64 ( Ingram, 2002), and it was even higher in American English children who were 24-36 months old with an average of 82%, reaching 94% in children 36 months old ( Watson & Terrel, 2012). This can be explained by the intricate and expansive consonantal system in Arabic, encompassing 28 consonants, meaning that children make more deletions and substitutions. This contrasts with Finnish, which has 13 consonants, and English, which has 24 consonants. Additionally, Arabic is a concatenative language, exposing children to a considerable number of words, many of which are multisyllabic. The study highlights the prevalence of error patterns in multisyllabic words. Age is a crucial factor in the development of TD children but not for the children with phonological disorders. That is, the older TD group had significantly higher scores in the PMLU, PWP and PC measures than the younger group. This suggests that children’s phonological system is in progress and that speech errors might need some time to be suppressed. The two groups had a largely adult-like phonological system and children encountered few difficulties. However, no significant difference was reported between the two TD groups based on PWC. The PWC tool counts mispronunciation of an individual word as one error regardless of the number of errors in that word, unlike the other three measures which compute the number and proportion of errors in every word. This may suggest that the younger age group scored less PMLU, PWP, and PCC errors compared to the older age group because of the high number of errors they made within the same word. This can be attributed to the discrepancies between the two groups in response to phonologically complex words.
Universally, children are believed to go through distinct stages reflecting the progress of their cognitive abilities (Mcleod, 2018). Huneety et al. (in progress) demonstrated that the mean PMLU scores for TD Arabic children aged 1;7-2;0 years stood at 4.9, experiencing a notable increase to 6.28 by 2;7-3 years. Furthermore, the PWC scores for children aged 2;7-3;0 were nearly three times higher than those of 1;7-2;0-year-olds. This observed trend correlated with the preservation of word structure and the expansion of their sound repertoire, leading to a corresponding rise in PMLU scores. Likewise, Beers et al. (2019) found a significant increase in PMLU values when the researchers investigated the phonological development of TD Dutch children aged from 1;3 to 4;0 years. Throughout the nine age stages, the mean PMLU values ranged from 3.94 to 5.40 points, with the most substantial growth occurring between 15-month-old children and their 23-month-old peers. By contrast to the TD Dutch children, children with phonological impairments scored comparable values on the same PLMU measure. This indicates that, without appropriate intervention and language therapeutic treatment for this vulnerable group of children, phonological progress may be limited and not improved by the child age. This observation coincides with findings of previous studies emphasizing that age does not play a crucial role in the language acquisition of impaired children. For example, Polite and Leonard (2006) employed Ingram’s phonological mean length of utterance as the basis for matching a group of preschoolers with SLI to TD peers. The study investigated the performance of three different groups of children: Ten 4;2-6;9-year-old children diagnosed with SLI, ten TD children comparable with the first group of children in their age and gender; and eight 2;9-5;0-year-old TD children with an average age of 3;6 years. Results revealed a significant main effect for the participant group; with a higher mean score for the TD older children compared to the SLI and TD younger groups. Additionally, the scores for the TD younger children were significantly higher than those of the children with SLI. This observation underscores the critical role of intervention in promoting language development among children with phonological impairment. These findings can be valuable for SLPs in their clinical endeavor to diagnose children with phonological disorders and make informed therapeutic decisions.
CONCLUSION & CLINIC IMPLICATION
The findings of the present study introduce valuable implementation for language clinicians and speech pathologists engaged in the diagnosis and treatment of children with phonological disorders. Identifying a child’s developmental stage is essential for the assessment process, involving a comparison of their scores with age-matched TD peers. This comparative analysis assists specialists in recognizing children with atypical phonological development and in providing a benchmark for monitoring their progress in therapy. Consequently, clinicians and SLPs can accurately diagnose phonological disorders and track therapeutic advancements using these findings. Notably, no scoring differences were observed between the older and younger age groups within the children with phonological disorders. This finding suggests that speech pathologists should not delay therapeutic interventions based solely on the child’s age but should initiate therapy promptly upon diagnosing phonological impairment.
As JA children’s linguistic abilities are primarily assessed through articulation tests due to the absence of tools like MLU, relying solely on articulation tests is insufficient for diagnosing children with articulation and/or phonological disorders. Morrison and Shriberg (1992) assert that single-word testing does not provide typical or optimal measures of speech performance. The study thus highly recommends an integrated model of whole-word measures (PMLU, PWP, and PWC) besides the segmental measure (PCC). A recommended practice involves obtaining a representative sample of at least 50 utterances for both quantitative and qualitative analyses of spontaneous speech samples through the four measures. However, speech pathologists should encourage children to produce words with diverse phonological structures and complexities, recognizing that performance scores depend on the phonological characteristics of words. For instance, children with phonological disorders may exhibit a tendency to delete weak syllables more frequently in multisyllabic words than in monosyllabic and disyllabic words. Future research can further explore the effectiveness of these measures in evaluating the phonological abilities of various groups of impaired children.
Notes
1) The primary rationale for employing the four measures was to ensure the comprehensiveness and efficacy of our assessment, providing speech pathologists with a holistic understanding of children’s phonological development. Each measure captures distinct aspects, including phonological complexity, word production, and overall speech accuracy. Additionally, while we acknowledge that, in general, the relationships among these measures might be expected due to their shared focus on articulation and phonological outcomes, it is crucial to emphasize that this study represents the first investigation of these measures within the context of Arabic phonology. Languages can exhibit unique features and complexities, and the interactions among these measures may vary (cf. Saaristo-Helin, Savinainen-Makkonen, & Kunnari, 2006; Taelman et al., 2005). 2) All MANOVA assumptions were checked using preliminary tests. Five of the six MANOVA assumptions were met: absence of univariate and multivariate outliers, multivariate normality, absence of multicollinearity, linearity, and homogeneity of variance. The homogeneity of covariance assumption was violated. However, we do not worry much about this violation as we continued the analysis with Pillai’s multivariate statistics instead of Wilk’s statistics.
Figure 1.
A boxplot of PMLU by age group and language development. 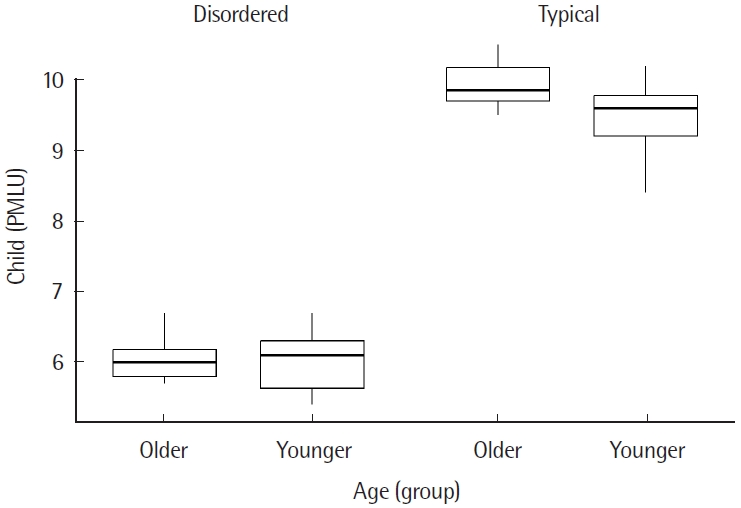
Figure 2.
A boxplot of PWP by age group and language development. 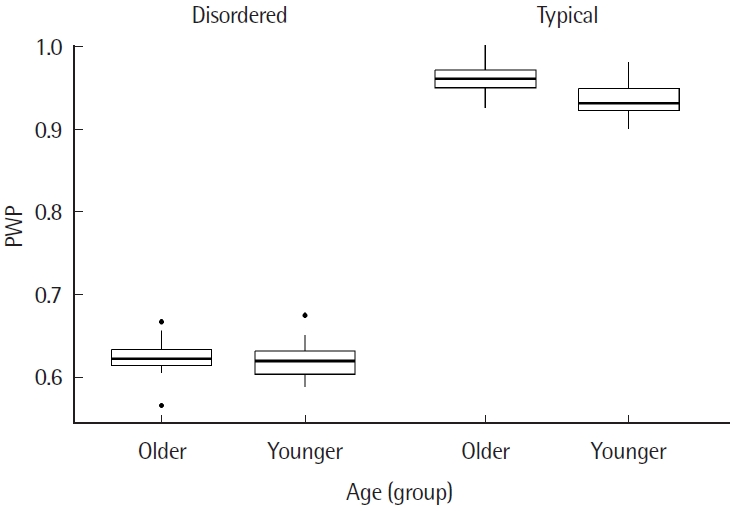
Figure 3.
A boxplot of PCC by age group and language development. 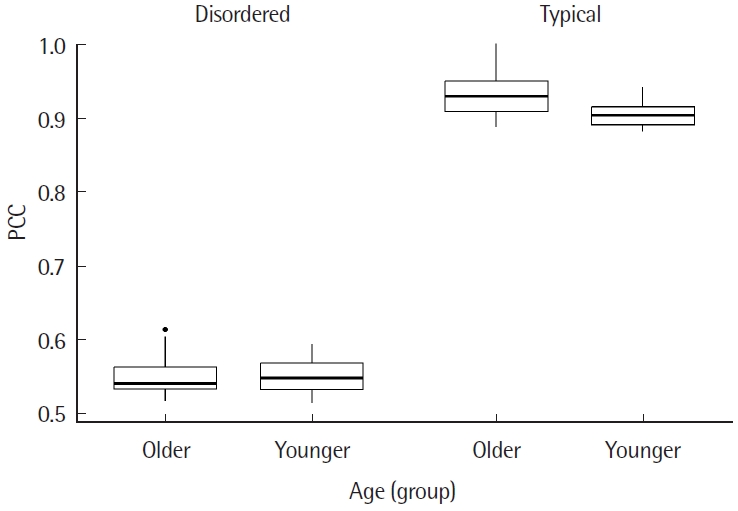
Figure 4.
A boxplot of PWC by age group and language development. 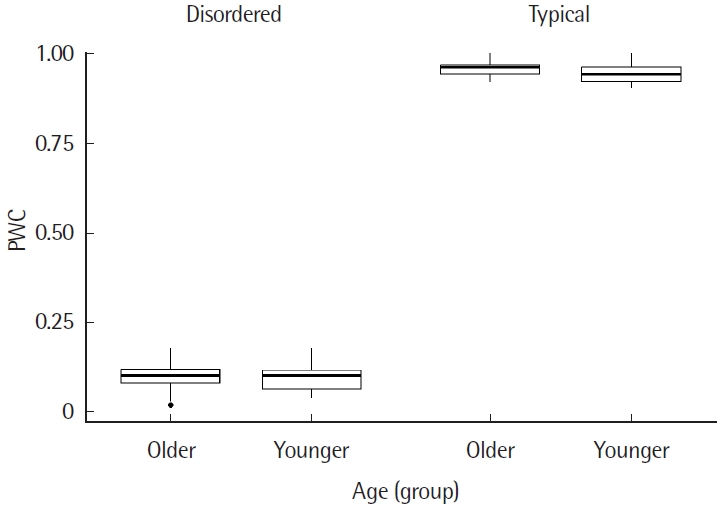
Table 1.
Means, SDs and ranges of the participants’ scores based on child language development, child group age and task
|
Task |
Language development |
Group age |
Mean (SD) |
Range |
|
Child PMLU |
Typical |
Younger |
9.49 (.444) |
8.4-10.2 |
|
Older |
9.94 (.302) |
9.5-10.5 |
|
Disordered |
Younger |
6.02 (.400) |
5.4-6.7 |
|
Older |
6.03 (.277) |
5.7-6.7 |
|
PWP |
Typical |
Younger |
.933 (.019) |
.899-.98 |
|
Older |
.959 (.019) |
.924-1 |
|
Disordered |
Younger |
.620 (.022) |
.587-.674 |
|
Older |
.622 (.020) |
.565-.666 |
|
PCC |
Typical |
Younger |
.906 (.016) |
.882-.942 |
|
Older |
.933 (.030) |
.887-1 |
|
Disordered |
Younger |
.550 (.024) |
.513-.593 |
|
Older |
.549 (.026) |
.516-.613 |
|
PWC |
Typical |
Younger |
.942 (.028) |
.9-1 |
|
Older |
.092 (.035) |
.92-1 |
|
Disordered |
Younger |
.956 (.022) |
.04-.18 |
|
Older |
.097 (.040) |
.02-.18 |
Table 2.
Type II MANOVA tests: Pillai’s trace test statistic
|
Variable |
Test stat |
F
|
Hypothesis df |
Error df |
Pr (> F) |
|
Language development |
.99488 |
3,935.7 |
4 |
81 |
< 2e-16***
|
|
Age group |
.14942 |
3.6 |
4 |
81 |
.01*
|
|
Language development*Age Group |
.13929 |
3.3 |
4 |
81 |
.015*
|
Table 3.
Pillai’s trace post hoc comparisons of the combined measure score for each group of participants
|
Group 1 |
Group 2 |
Test stat |
F
|
Hypothesis df |
Error df |
Pr (> F) |
|
Younger typical |
Younger disordered |
.990 |
1,930 |
4 |
81 |
< .001***
|
|
Older typical |
Older disordered |
.990 |
2,008 |
4 |
81 |
< .001***
|
|
Younger typical |
Older typical |
.249 |
6.713 |
4 |
81 |
< .001***
|
|
Younger disordered |
Older disordered |
.06 |
.122 |
4 |
81 |
.974 |
Table 4.
Tests of ANOVAs for each testing measure by child language development and child group age
|
Source |
Dependent variable |
df |
Mean square |
F-value |
p-value |
|
Language development |
PLMU |
1 |
299.333 |
2,283.833 |
< .001***
|
|
PWP |
1 |
23,288.553 |
5,777.791 |
< .001***
|
|
PCC |
1 |
30,030.374 |
4,957.272 |
< .001***
|
|
PWC |
1 |
160,654.545 |
15,716.760 |
< .001***
|
|
Age group |
PLMU |
1 |
1.159 |
8.844 |
.004**
|
|
PWP |
1 |
44.916 |
11.144 |
.001**
|
|
PCC |
1 |
38.188 |
6.304 |
.014*
|
|
PWC |
1 |
20.045 |
1.961 |
.165 |
|
Language development* Age group |
PLMU |
1 |
1.026 |
7.825 |
.006**
|
|
PWP |
1 |
31.596 |
7.839 |
.006**
|
|
PCC |
1 |
43.640 |
7.204 |
.009**
|
|
PWC |
1 |
4.545 |
0.445 |
.507 |
Table 5.1.
Post hoc comparisons of child PMLU scores for each group of participants
|
Group 1 |
Group 2 |
Estimate |
Lower bound |
Upper bound |
p. adj |
|
Younger typical |
Younger disordered |
3.472 |
3.215 |
3.729 |
< .001***
|
|
Older typical |
Older disordered |
3.904 |
3.728 |
4.080 |
< .001***
|
|
Younger typical |
Older typical |
-.445 |
-.677 |
-.213 |
< .001***
|
|
Younger disordered |
Older disordered |
-.013 |
-.223 |
.196 |
.896 |
Table 5.2.
Post hoc comparisons of child PWP scores for each group of participants
|
Group 1 |
Group 2 |
Estimate |
Lower bound |
Upper bound |
p. adj |
|
Younger typical |
Younger disordered |
.313 |
.301 |
.326 |
< .001***
|
|
Older typical |
Older disordered |
.337 |
.325 |
.349 |
< .001***
|
|
Younger typical |
Older typical |
-.026 |
-.037 |
-.014 |
< .001***
|
|
Younger disordered |
Older disordered |
-.002 |
-.015 |
.01 |
.718 |
Table 5.3.
Post hoc comparisons of child PCC score for each group of participants
|
Group 1 |
Group 2 |
Estimate |
Lower bound |
Upper bound |
p. adj |
|
Younger typical |
Younger disordered |
.355 |
.343 |
.368 |
< .001***
|
|
Older typical |
Older disordered |
.384 |
.366 |
.401 |
< .001***
|
|
Younger typical |
Older typical |
-.027 |
-.042 |
-.012 |
< .001***
|
|
Younger disordered |
Older disordered |
.009 |
-.014 |
.016 |
.904 |
Table 6.
Correlations between the measure scores for each language development group
|
Measure |
Group |
PMLU |
PWP |
PCC |
PWC |
|
PMLU |
Typical |
- |
.49***
|
.34*
|
.38**
|
|
Disordered |
- |
.55***
|
.71***
|
.35*
|
|
PWP |
Typical |
- |
- |
.75***
|
.60***
|
|
Disordered |
- |
- |
.44**
|
.45**
|
|
PCC |
Typical |
- |
- |
- |
.58***
|
|
Disordered |
- |
- |
- |
.31*
|
Table 7.
Summary of children’s phonological processes
|
The phonological process |
Definition |
Underlying form |
Surface form |
Gloss |
|
De-emphasis |
An emphatic sound loses the secondary pharyngealization characteristic (Alqattan, 2015) |
sˤu:sˤ |
su:s |
Chick |
|
Sound substitution/distortion |
Replacing a sound with an easier alternative |
bar.ra |
bal.la |
Outside |
|
A sound distortion refers to abnormal sound changes, i.e., when the speaker produces a sound in a manner that deviates from the typical way of articulating a particular sound (Bauman-Waengler, 2008) |
|
Weak syllable deletion |
The process of deleting an unstressed syllable in a multisyllabic word (Bauman-Waengler, 2008) |
bur.tu.’ꝗꭤ:.leh |
but.’tꭤ:.leh |
An orange |
|
Syllable simplification by Cluster reduction |
A cluster is simplified into a single consonant (Bauman-Waengler, 2008) |
kalb |
kabb |
Dog |
|
Syllable simplification by final consonantdeletion |
A process of omitting consonants in final positions (Bauman-Waengler, 2008) |
ma.ḥru:g |
ma.ḥru: |
Burned |
REFERENCES
Abu Guba, M. N. (2021). Consonant gemination within English loanwords in Ammani Arabic: an Optimality-Theoretic analysis. Journal of Linguistics, 57(1), 1–38.
Alqattan, S. (2015). Early phonological acquisition by Kuwaiti Arabic children. (Doctoral dissertation). Newcastle University, Newcastle upon Tyne, England.
Amayreh, M. M., & Dyson, A. T. (1998). The acquisition of Arabic consonants. Journal of Speech, Language, & Hearing Research, 41(3), 642–653.   Amayreh, M. M., & Dyson, A. T. (2000). Phonetic inventories of young Arabic-speaking children. Clinical Linguistics & Phonetics, 14(3), 193–215. Ayyad, H. S. (2011). Phonological development of typically developing Kuwaiti Arabic-speaking preschoolers. (Doctoral dissertation). University of British Columbia, Vancouver, Canada.
Bauman-Waengler, J. (2008). Articulatory and phonological impairments: a clinical focus Boston, MA: Pearason Education.
Beers, M., Rodenburg-Van Wee, M., & Gerrits, E. (2019). Whole-word measures and the speech production of typically developing Dutch children. Clinical Linguistics & Phonetics, 33(12), 1149–1164. Bernthal, J. E., & Bankson, N. W. (2009). Articulation and phonological disorders (6th ed.) Boston: Pearson.
Bónová, I., Slancová, D., & Mikulajová, M. (2005). The measurement of phonological acquisition in Slovak. Proceedings of the 10th International Congress for the Study of Child Language, Berlin.
Burrows, L., & Goldstein, B. A. (2010). Whole word measures in bilingual children with speech sound disorders. Clinical Linguistics & Phonetics, 24(4-5), 357–368. Eads, A., Khater, J., & Mielke, J. (2018). Arabic L2 phonological acquisition: An ultrasound study of emphatics and gutturals 1. In W. Alhawary (Ed.), The Routledge handbook of Arabic second language acquisition. 93–112. Routledge.
Dyson, A. T., & Amayreh, M. M. (2000). Phonological errors and sound changes in Arabic-speaking children. Clinical Linguistics & Phonetics, 14(2), 79–109. Farquharson, K., Hogan, T. P., & Bernthal, J. E. (2014). The impact of phonological awareness training on phonological short-term memory skills in prekindergarten and kindergarten children, Language, Speech, & Hearing Services in School, 45(4), 265–277.
Fey, M. E. (1992). Articulation and phonology: inextricable constructs in speech pathology, Language, Speech, & Hearing Services in School, 23(3), 225–232.
Fox, J., & Weisberg, S. (2019). An R companion to applied regression. (Third edition). Sage, Thousand Oaks CA.
Gerrits, E., & de Bree, E. (2009). Early language development of children at familial risk of dyslexia: speech perception and production. Journal of Communication Disorders, 42(3), 180–194. Grunwell, P. (1987). Clinical phonology (2nd ed.) Baltimore, MD: Williams & Wilkins.
Ha, S. (2022). Phonological error patterns in subgroups of speech sound disorders. Communication Sciences & Disorders, 27(3), 647–657. Hamdan, J. M., & Amayreh, M. M. (2007). Consonant profile of Arabic speaking school-age children in Jordan. Folia Phoniatrica et Logopaedica, 59(2), 55–64. Holm, A., & Dodd, B. (1999). An intervention case study of a bilingual child with phonological disorder. Child Language Teaching & Therapy, 15(2), 139–158. Huneety, A. I., Mashaqba, B. M., Al-Shdifat, K. G., Khasawneh, E. A., & Thnaibat, B. (2023). Multisyllabic word production by Jordanian Arabic speaking children. Speech, Language & Hearing, 26(4), 249–265. Huneety, A., Khashashneh, N., Mashaqba, B., Guba, M. N. A., & Alshdaifat, A. (2023). Phonological abilities of children with dyslexia in jordan: a whole-word approach. Eurasian Journal of Applied Linguistics, 9(3), 21–32.
Huneety, A., Mashaqba, B. M., Al-Shdifat, K. G., Abu Guba, M., & Al-Deaibes, M. (in progress). Phonological mean length of utterance in Arabic.
Ingram, D. (1981). Procedures for the phonological analysis of children’s language Baltimore: University Park Press.
Ingram, D. (1989). First language acquisition: method, description and explanation Cambridge University Press.
Ingram, D. (2002). The measurement of whole-word productions. Journal of Child Language, 29(4), 713–733. Ingram, D., & Ingram, K. D. (2001). A whole-word approach to phonological analysis and intervention. Language, Speech, & Hearing Services in School, 32(4), 271–283. Kumar, B. R., & Bhat, J. S. (2009). Phonological mean length of utterance (PMLU) in Kannada-speaking children. Language in India, 9(8), 489–502.
Larrivee, L. S., & Catts, H. W. (1999). Early reading achievement in children with expressive phonological disorders. American Journal of Speech-Language Pathology, 8(2), 118–128. Mashaqba, B. M., Al-Shdifat, K. G., Al Huneety, A. I., Alhala, M. A., Mashaqba, B. M., Al-Shdifat, K. G., & Alhala, M. A. (2019). Acquisition of syllable structure in Jordanian Arabic. Communication Sciences & Disorders, 24(4), 953–967. Mashaqba, B., Huneety, A., Al-Khawaldeh, N., & Thnaibat, B. (2021). Geminate acquisition and representation by Ammani Arabic-speaking children. International Journal of Arabic-English Studies, 21(1), 219–242. Mashaqba, B., Daoud, A., Zuraiq, W., & Huneety, A. (2022). Acquisition of emphatic consonants by Ammani Arabic-speaking children. Language Acquisition, 29(4), 441–456. Mashaqba, B., Huneety, A., Abu Guba, M. A., & Al-Duneibat, B. A. (2022). Production of gutturals by non-native speakers of Arabic. Indonesian Journal of Applied Linguistics, 12(2), 334–347. Mashaqba, B., Huneety, A., Al-Khawaldeh, N., Al-Deaibes, M., & Zeidan, Z. (2023). Acoustics of long vowels in Arabic-speaking children with hearing impairments. Humanities & Social Sciences Communications, 10(1), 1–11. Morrison, J. A., & Shriberg, L. D. (1992). Articulation testing versus conversational speech sampling. Journal of Speech, Language, & Hearing Research. 35(2), 259–273.
Polite, E. J., & Leonard, L. B. (2006). Finite verb morphology and phonological length in the speech of children with specific language impairment. Clinical Linguistics & Phonetics, 20(10), 751–760. Saaristo-Helin, K. (2011). Phonological mean length of utterance as an indicator of typical and impaired phonological development in children acquiring Finnish. (Doctoral dissertation). University of Helsiniki, Turku, Finland.
Saaristo-Helin, K., Savinainen-Makkonen, T., & Kunnari, S. (2006). The phonological mean length of utterance: methodological challenges from a crosslinguistic perspective. Journal of Child Language, 33(1), 179–190. Shriberg, L. D., & Kwiatkowski, J. (1982). Phonological disorders III: a procedure for assessing severity of involvement. Journal of Speech & Hearing Disorders, 47(3), 256–270.
Smith, N. V. (1973). The acquisition of phonology: a case study Cambridge University Press.
So, L. K., & Dodd, B. J. (1995). The acquisition of phonology by Cantonesespeaking children. Journal of Child Language, 22(3), 473–495. Taelman, H., Durieux, G., & Gillis, S. (2005). Notes on Ingram’s whole-word measures for phonological development. Journal of Child Language, 32(2), 391–405. Watson, J. C. (2002). The phonology and morphology of Arabic OUP Oxford.
Watson, M. M., & Terrell, P. (2012). Longitudinal changes in phonological whole-word measures in 2-year-olds. International Journal of Speech-Language Pathology, 14(4), 351–362. Wickham, H., Averick, M., Bryan, J., Chang, W., McGowan, L. D. A., François, R., ..., & Yutani, H. (2019). Welcome to the Tidyverse. Journal of Open Source Software, 4(43), 1–6. Yavaş, M., & McLeod, S. (2010). Speech development and disorders:a multilingual and cross-linguistic perspective Multilingual Matters.
Zhu, H., & Dodd, B. (2000). Phonological disorders in Chinese children: a perceptual and acoustic study. Clinical Linguistic & Phonetics, 14, 165–191.
|
|